Dental caries remains a significant public health issue among children under six, highlighting the need for behavioral strategies to lower individual risk and address disparities in early childhood caries. Preventive measures like the twice-daily use of fluoridated toothpaste (Touger-Decker, 2013), adherence to a diet low in cariogenic substances, and promoting healthy feeding behaviors (Hirsch et al., 2012) are crucial. However, traditional treatments such as fillings and generic advice on tooth brushing and diet fail to target the specific behavioral risks leading to high recurrence rates (Lumsden et al., 2019). MySmileBuddy (MSB) program introduces a novel approach by focusing on individualized, family-centered support through the use of apps, widgets, and videos to encourage healthy behaviors, such as replacing sugary snacks with healthier options, with the aid of community health workers (Lumsden et al., 2021).
Target audience for MSB are families with children aged 0-18, and their motivation and readiness to engage with their own oral healthcare is varied. Parents and caregivers have diverse educational levels and parents in low SES often suffer from poor oral healthcare themselves. This may be due to a variety of social and environmental barriers to good oral health, including low incomes, oral health knowledge, limited access to healthy foods, and transportation challenges.
However, the application is primarily targeted at adult caregivers which often excludes children as their own healthcare partner. This project presents a design that engages children as the active participants in a family-based oral health behavior change program. The need was identified during user testing. First, a hybrid mode of engagement was asked to better facilitate shared experiences and communication across family members, especially with young children. Children need to be active participant in their own oral healthcare process, developing their agency and life-long habit.
This MSB program is deeply rooted in the principles of Social Cognitive Theory and the Health Belief Model which are instrumental in effecting behavior change (Ismail et al., 2011). Based on these theories, MSB has developed and implemented a behavioral change model encapsulated by four sequential stages: education, assessment, behavior, and follow-up. The program itself serves as a supportive environmental factor for the initiation and maintenance of healthy behavioral changes within the challenging daily contexts of families (Lumsden et al., 2021). This comprehensive approach is designed to catalyze and maintain behavior changes, thereby contributing to the reduction of dental caries among children (Lumsden et al., 2021).
In order to engage children as active participants, two design approaches were integrated, storytelling through graphic novel and gamification of behavioral change process. Gamification refers to the use of design elements characteristic for games in non-game contexts (Deterding et al., 2011). A systematic review of mobile applications that include gamification for children’s oral health education provides a table with exemplary gamification features suitable for oral hygiene education, which serves as the framework for our solution (Fijačko et al. 2020). The review concludes that gamification features with evidence-based dentistry have good potential for behavioral change in the form of learning, performing, and maintaining proper oral health (Fijačko et al., 2020). In addition, using gamification features to target parents is conducive to their children’s oral health with greater behavioral change ( Zolfaghari et al. 2021). Therefore, we propose the incorporation of gamification on the bilateral parent-children interaction regarding oral health to enhance learning outcomes and behavioral change. Zolfaghari
Family plays a crucial role in addressing dental health issues among children (Berger & Font, 2015). Not only can they model and reinforce positive dental hygiene habits such as regular brushing and flossing, but they can also make informed decisions regarding their children's nutritional intake, limiting sugary snacks and drinks that contribute to dental problems. Recognizing the important role of family, the inclusive design of MySmileBuddy (MSB) incorporates a family-based learning approach through the lens of constructivism, encouraging children and their families to actively participate in dental health-related activities, discussions, and goal setting and decision-making processes (Vygotsky, 1978). Through these interactive experiences, family members co-construct knowledge about dental health management, good practices, and healthy behaviors.
Building on the principles of constructivism, the MSB inclusive design introduces features aimed at fostering autonomy among children in their learning journey (Jonassen, 1991). They allow them to establish personal goals, monitor their progress, and receive rewards or badges for consistent oral health practices. Additionally, it offers opportunities for them to partake in making decisions about their dental health goals. The primary objective of these features is to transform children from passive recipients of information into active participants in their healthcare, thereby empowering them and instilling a sense of ownership over their oral health.
To complement the active engagement of children in their dental healthcare, the design further enhances the role of parents by equipping them with the tools to support their children’s learning journey. This includes providing guidance, support, and clear instructions to foster good dental health practices. Such an approach not only empowers parents to be effective facilitators in their children's health education but also strengthens the collaborative dynamic within the family, ensuring a cohesive effort towards achieving optimal oral health.
MSB, the behavioral change approach to caries management has been developed over 10 years through iterations of design and research in collaboration between subject-matter experts and learning experiences designers. With recognition to engage children as the active participants in their own oral health behavior, we designed graphic novels and games to engage children in the behavioral change approach of the overall program: education, assessment, behavior, and follow-up.
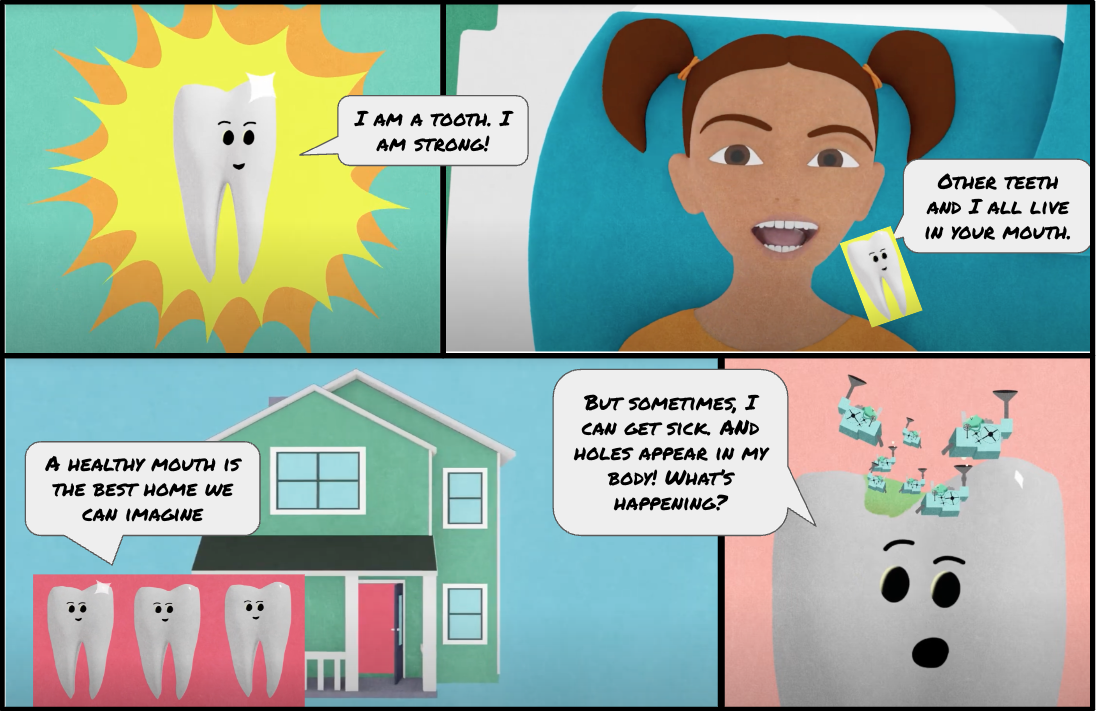
To educate and actively engage children in dental health, two graphic novels were developed titled "The Surprising True Story of Cavities," targeted at two distinct age groups: 0-8 and above 9. These novels, while consistent in content, are tailored in language style and complexity to suit the respective audiences. The narrative illustrates the battle of a tooth against bacteria machines, detailing how it halts acid production and repairs cavities with the support of fluoride toothpaste. The creation of these graphic novels was informed by informational videos we had previously produced and integrated into the MSB experience through collaboration with oral healthcare experts. This ensured that the learning objectives, promoted behaviors, and key terminologies remained scientifically accurate and aligned with MSB's educational goals.
In leveraging the power of storytelling and immersion, we endowed each character with a distinct personality, aiming to captivate and educate simultaneously (see Figure 1). To reduce extraneous cognitive load (Sweller et al., 1998), the story element contributes to an understanding of the scientific processes underlying tooth decay and repair, thus serving the dual purpose of entertaining and educating.
Figure1
Example of graphic novel for children 0-8 years old
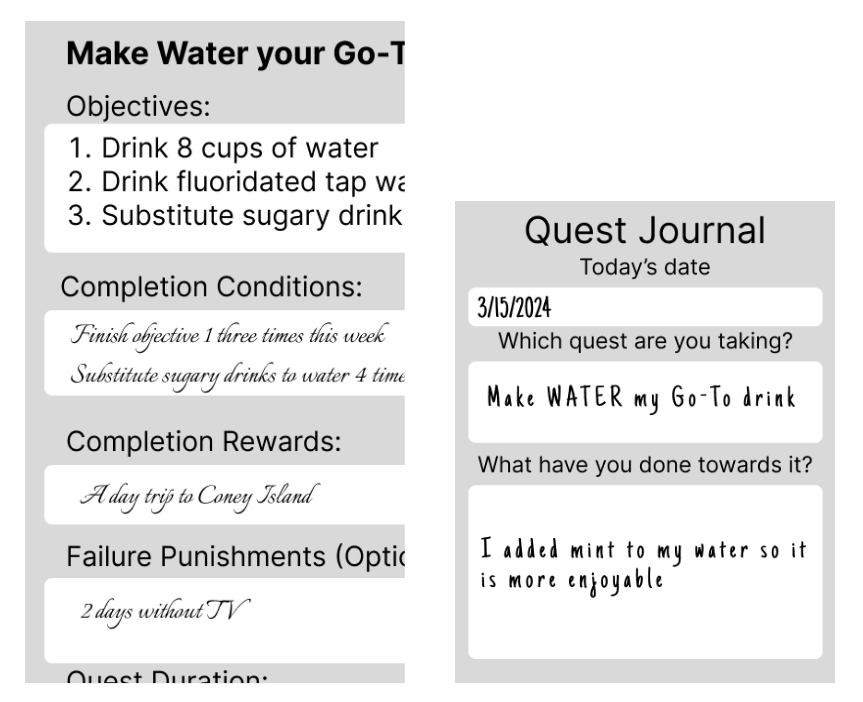
Based on Fijačko et al.’s (2020) exemplary gamification features, goals, ownership, badges, meaning, loss aversion, fantasy, social facilitation, and ideological incentives were integrated into the design of gamified experience addressing behavior and follow-up phases of behavioral change model. Clear goals and action plans selected by the family are gamified through “obfuscating” and “distancing” to integrate educational tips. Game mechanics and artifacts integrate knowledge and behavioral strategies to address their motivational and behavioral enables and barriers. In the gamified model, a caregiver such as a parent would assume the role of quest master, facilitating the game. The quest master supports the player as they decide on the quest and monitor their progress. The educational content and action plan for healthy habit is integrated as part of the quest and game mechanics (see Figure 2) so engaging in the gameplay automatically engages the player in the educational and behavioral change journey.
Figure 2
Game rule and quest cards
While family-based healthcare intervention is found to be an effective way to address children’s oral healthcare, providing opportunities for children to take control and ownership of their own healthy behavior can be a powerful means for lifelong behavioral change. Game-based and narrative-based approach to education and behavioral change support can be an effective instructional approach to address this goal.